Data Insight: Communication Failures in Inpatient Diagnostic Claims Involving Nursing
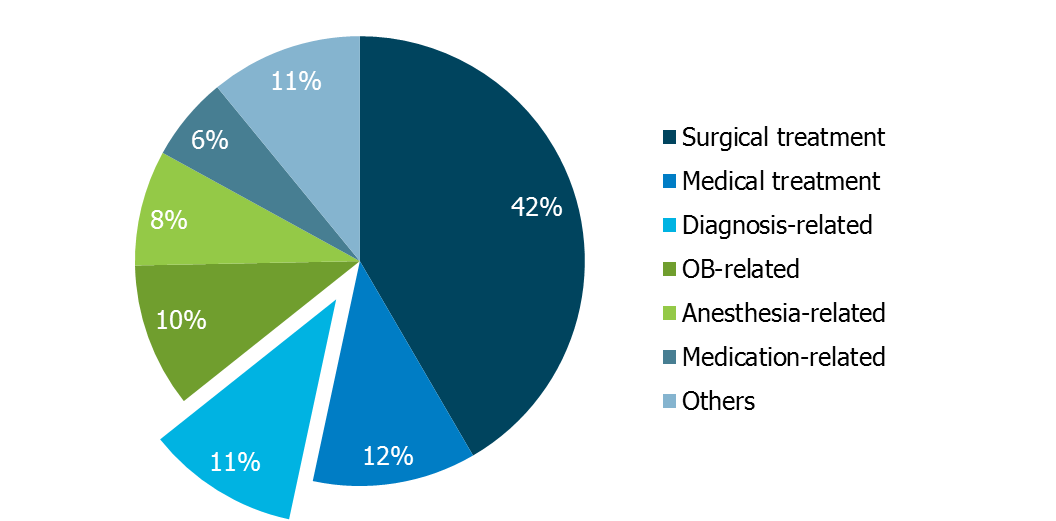
Diagnosis-related allegations are the third most frequent inpatient hospital claim type (Figure 1). Although medicine and surgical specialties typically are noted as the responsible service, nursing staff are identified as either primarily or secondarily responsible in 22 percent of these claims.
Figure 1. Allegation Categories in Inpatient Claims
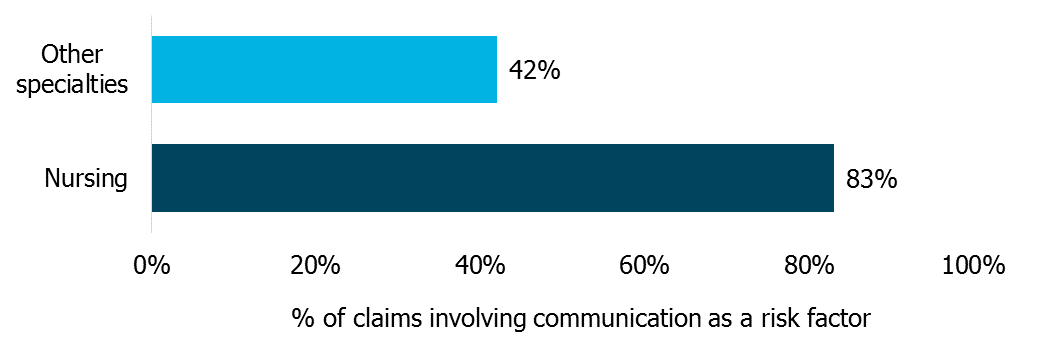
Of the nursing-involved claims, more than 75 percent resulted in a severe patient outcome (i.e., permanent disability or death). Further, these claims were more costly than other inpatient diagnostic claims, and almost all of them involved a critical communication failure (Figure 2).
Figure 2. Communication as a Risk Factor in Inpatient Diagnosis-Related Claims
Examples of the nursing communication problems noted in inpatient diagnostic claims include:
- Failure to appreciate the significance of postcardiac catheterization abdominal pain, resulting in delayed diagnosis of a retroperitoneal hemorrhage and subsequent patient death
- Failure to notify the nursing supervisor and physician of a patient’s fall and subsequent pain, resulting in delayed diagnosis of a spinal cord compression and permanent lower extremity paralysis
- Failure to report an orthopaedic patient’s complaint of significant leg pain and swelling and increased blood pressure, resulting in an emergent surgery to relieve compartment syndrome
- Assumption that a patient’s severe headache was due to known migraines, resulting in delayed diagnosis of a hemorrhagic stroke and subsequent patient death
Case Illustration
A male patient in his late forties presented to an emergency department with complaints of lower back pain that occurred while sitting and standing. The nurse documented that the patient “can’t get up,” but did not document the reason why. Upon the patient’s admission for neurological assessment, a nurse performed an initial evaluation and documented that the patient lacked sensation from the waist down, but she did not tell the neurologist (later, the nurse stated that she did not feel like the lack of sensation was a new finding).
Eight hours after the patient’s admission, the same nurse documented that the patient had no response to touch on his foot, but she still did not inform the physician. One hour later, a second nurse noted that the patient was incontinent and called the physician. An order for a nonemergent MRI was changed to a STAT order.
The patient was subsequently diagnosed with acute cauda equina syndrome and underwent bilateral partial hemilaminectomy, medical fasciotomy, and foraminotomy, followed by a second surgery for anterior cervical decompression and arthrodesis. The patient was left with diminished lower extremity function and neurogenic bladder.
Key Points
- Communicate significant changes in a patient’s condition to the provider responsible for the patient’s care. Communication should occur in timeframes set forth in organizational policy.
- Ensure prompt communication of critical tests results and findings to the appropriate provider(s).
- Don’t make assumption-based decisions — e.g., “This new symptom is just another manifestation of what is already known.” Assumptions can result in lost opportunities for timely diagnosis and treatment.
- Follow requirements for using tools, checklists, and forms as part of the communication and care coordination process.
Resources
Data Source
MedPro Group closed claims data, 2007–2016
